Another option is surgery to remove the spleen called a splenectomy. The more commonly used treatments along with their.
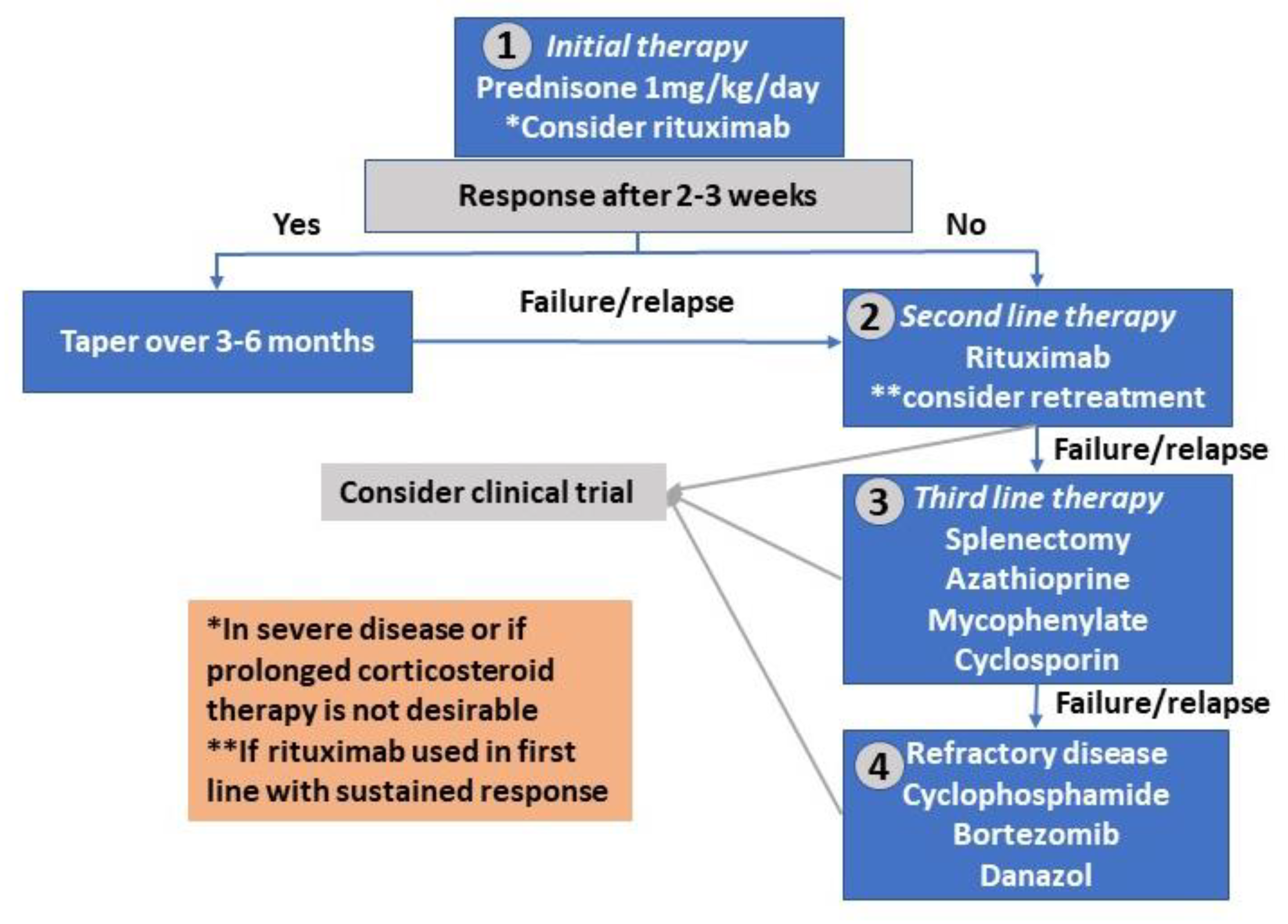
![]() Transition From Chronic Relapsing Autoimmune Hemolytic Anemia Aiha Download Scientific Diagram
Transition From Chronic Relapsing Autoimmune Hemolytic Anemia Aiha Download Scientific Diagram
This is because of significant differences in the rates of hemolysis and associated diseases and because there is considerable clinical heterogeneity.
How i treat warm autoimmune hemolytic anemia. Microangiopathic hemolytic anemia MAHA refers to a subgroup of hemolytic anemia where there is fragmentation and hemolysis due to damage of erythrocytes in the small blood vessels. Primary warm antibody autoimmune hemolytic anemias respond well to steroids but most patients remain steroid-dependent and many require second-line. Warm AIHA due to antibodies that are active at body temperature is the most common type of AIHA.
Further evidence of hemolysis may include a reticulocytosis raised lactate dehydrogenase LDH low or. This is because of significant differences in the rates of hemolysis and associated diseases and because there is considerable clinical heterogeneity. In addition there is a lack of clinical trials required to refine and.
Daratumumab in life-threatening autoimmune hemolytic anemia following hematopoietic stem cell transplantation. Treatment decisions should be based on careful diagnostic evaluation. Treatment depends on the type of antibody causing the anaemia.
Autoimmune hemolytic anemia is a heterogeneous disease with respect to the type of the antibody involved and the absence or presence of an underlying condition. Antibody-dependent cell-mediated cytotoxicity by macrophagesactivated lymphocytes occurs in the lymphoid organs and spleen extravascular hemolysis. In one study warm AIHA represented 703 percent of the cases of AIHA that were encountered.
We combined these results with a review of 36 cases of AIHA treated with IVGG reported in the literature. Until now treatment of primary autoimmune hemolytic anemia of the warm type wAIHA is primarily based on immunosuppression. Autoimmune hemolytic anemia AIHA is an uncommon entity that presents diagnostic prognostic and therapeutic dilemmas despite being a well-recognized entity for over 150 years.
A high-dose of these drugs may be recommended initially followed by a gradual reduction tapering of the dose over the next few weeks or months. This topic reviews the evaluation and management of warm AIHA in adults. However many patients do not respond adequately to treatment and treated patients may develop severe side effects due to uncontrolled mixed andor long-lasting immunosuppression.
Antibody-dependent cell-mediated cytotoxicity by macrophagesactivated lymphocytes occurs in the lymphoid organs and. Antibody-dependent cell-mediated cytotoxicity by macrophagesactivated lymphocytes occurs in the lymphoid organs and spleen extravascular hemolysis. The ability of the bone marrow BM to compensate determines clinical.
Autoimmune hemolytic anemia AIHA is an uncommon entity that presents diagnostic prognostic and therapeutic dilemmas despite being a well-recognized entity for over 150 years. How I treat warm autoimmune hemolytic anemia. Similarly DAT negativity is not essential with controlled hemolysis.
If hemolysis continues that is well compensated after prednisone tapering starting a second-line treatment may not be necessary. Antibody-dependent cell-mediated cytotoxicity by macrophagesactivated lymphocytes occurs in the lymphoid organs and spleen extravascular hemolysis. Initial medical treatment consists of prednisone.
Erythropoietin may improve anemia in patients with autoimmune hemolytic anemia associated with reticulocytopenia. Corticosteroids and immunoglobulins are two commonly used treatments for warm antibody AIHA. Warm autoimmune hemolytic anemia wAIHA is caused by increased erythrocyte destruction by IgG autoantibodies with or without complement activation.
Not all people with warm type autoimmune haemolytic anaemia will need treatment but for those who do the first treatment is usually steroids. The ability of the bone marrow BM to compensate. Sixteen clinical variables were examined to determine associations.
Or 3 intolerance to a currently effective treatment. Rituximab is an artificially. Warm autoimmune hemolytic anemia AIHA is the most common type of AIHA.
It is characterized by the presence of red cell fragments or schistocytes on blood film review. Intravenous immunoglobulin G IVIG has been used for patients with AIHA but only a few patients have responded to this treatment and. Autoimmune hemolytic anemia AIHA is caused by autoantibodies that react with self red blood cells RBCs and cause them to be destroyed.
Warm autoimmune hemolytic anemia wAIHA is caused by increased erythrocyte destruction by immunoglobulin G IgG autoantibodies with or without complement activation. To determine whether warm-antibody autoimmune hemolytic anemia AIHA responds to treatment with intravenous gammaglobulin IVGG we conducted separate pilot studies at three institutions enrolling a total of 37 patients. The ability of the bone marrow BM to compensate.
The treatment of warm antibody hemolytic anemia is symptomatic and supportive. Warm autoimmune hemolytic anemia wAIHA is caused by increased erythrocyte destruction by immunoglobulin G IgG autoantibodies with or without complement activation. In addition there is a lack of clinical trials required to refine and.
Relapsehemoglobin11gdLorsymptomatic anemia withongoing evidence of hemolysis. Affected individuals are usually treated with corticosteroid drugs such as prednisone and can usually be well controlled with proper treatment. Warm AIHA can be idiopathic and a treatment plan related to managing anemia.
Other medicines which work on the immune system or rituximab might be used after steroids have been tried. Warm autoimmune hemolytic anemia wAIHA is caused by increased erythrocyte destruction by immunoglobulin G IgG autoantibodies with or without complement activation.